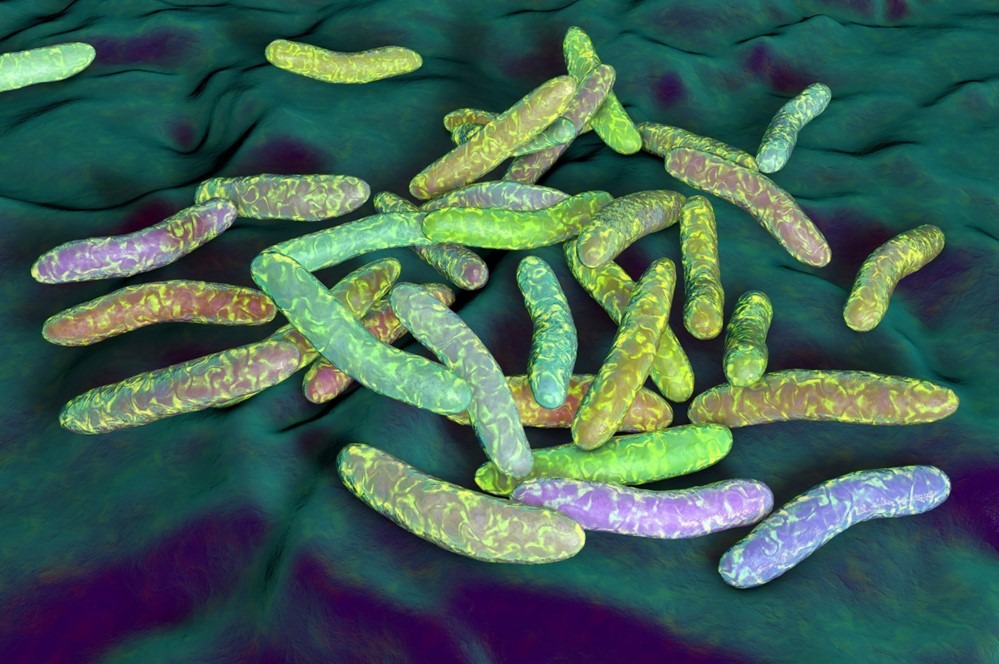
Holosystemics Part V: The Microeukaryotes of the Coral HolobiontMudskippers: Unique Amphibious GobiesHolosystemics Part IV: Dysbiosis and the Microscopic Coral AllianceHolosystemics Part III: The Prokaryotes of the Coral HolobiontFish Diversity: The Big PictureThe Zooxanthellae of the Hermatypic Coral HolobiontHolosystemics Part I: Captive Reef Function versus MalfunctionInterview with a Microbe Cultivator: Kenneth Wingerter of Hydrospace LLC on Aquarium ProbioticsInterview with the Aquaculture Professor: Dr. Michael A. Rice on Bivalves in the AquariumThe Hero Called Berghia: Noble Nudibranchs for Biocontrol of Aiptasia sp. in the Reef AquariumOysters in the Sump?! Redefining Biofiltration w/BivalvesClownfish ExplainedThe Frenatus Group